חומצות שומן חיוניות
מהן חומצות שומן חיוניות?
ישנן חומצות שומן רבות ומגוונות אך ניתן לחלקן ל 2 קבוצות עיקריות: "חומצות שומן רוויות" ו"חומצות שומן בלתי רוויות".
"החיוניות" נקראות כך משום שגופנו איננו יודע לסנתז אותן לבדו והוא חייב לקבלן מן המזון.
-
"חומצת שומן רוויה" – רוויה באטומי מימן שקשורים לכל אטומי הפחמן. חומצות שומן אלו נוטות להיות מוצקות בטמפרטורת החדר כגון במאכלים מעולם החי וגם בשמנים צמחיים מוקשים כגון מרגרינה.
-
"חומצת שומן בלתי רוויה" – חומצה שאיננה רוויה באטומי מימן. חומצות אלו נוטות להיות במצב צבירה נוזלי בטמפרטורת החדר כגון שמן זית בכבישה קרה, שמן דגים, שמן פשתן ועוד.
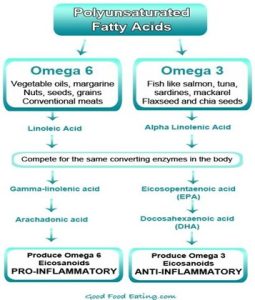
חומצות השומן נבדלות זו מזו ע"י הקשרים הכימיים שלהן בשרשרת. אם אחד הקשרים של הפחמן התחבר לאטום הפחמן שלפניו, ייווצר קשר כפול בין שני אטומי פחמן, ושני אטומי המימן שהיו מחוברים לשני אטומי הפחמן לא יתקיימו ואז תוגדר חומצת השומן ע"פ אזור הקשר. לדוגמה אם בין הקשר השלישי לרביעי בין אטומי הפחמן יהיה כפול אז השרשרת מקבלת את השם אומגה 3. ואם הקשר השישי הוא הכפול אז חומצת השומן תקרא אומגה 6 וכן הלאה.
דוגמאות נוספות לקשרים הפחמניים: ח. שומן אולאית נקראת אומגה 9. ח. שומן לאורית אומגה 12. ח. שומן פלמיטית נקראת אומגה 16. ח.שומן סטארית נקראת אומגה 18 וכ"ו.
חשוב לדעת שחומצות השומן הרוויות מגיעות אלינו בעיקר מעולם החי בעוד שחומצות השומן הבלתי רוויות מגיעות בעיקר מעולם הצומח.
2 חומצות השומן החיוניות שנסקור בלימוד זה הן אומגה 3 ואומגה 6. כיום עם התפתחות המדע אנו גם יודעים שעליהן להימצא בכמות וביחסים נכונים ביניהן (ראה טבלה בסוף).
תפקידים עיקריים אומגה 6 – חומצה לינולאית – Linoleic Acid.
-
שיפור תפקודי המח – מניעת מחלות דמנציה
-
הזנת מערכת העצבים – זיכרון וריכוז
-
תמיכה במערכת החיסון בלקיחה לאורך זמן
-
פעילות אנטי דלקתית רב מערכתית
-
איזון מערכת הורמונאלית בעיקר אצל נשים
-
טיפול ותמיכה במחלות עור כרוניות
-
פוריות גברים ונשים
שלב תוצר ביניים של פירוק אומגה 6 נותן לגופנו את חומצת השומן גמא-לינולאית אסיד (G.L.A) Gamma Linolenic Acid, אשר לה תכונות חשובות ביותר, העיקרית שבהן פעילות אנטי דלקתית. כיום אנו יודעים שמרבית המחלות הכרוניות (ממחלות מפרקים, מחלות עור כרוניות ועד סרטן) מתחילות בבסיסן בדלקת ברמה כלשהי בתא, וחומצת שומן זו מעודדת יצור חומרים הנקראים פרוסטגלנדינים (prostaglandin) מסוג PG1+PG3 הנחשבים לנוגדי דלקת ובתוך כך מעכבת את פעולת מתווכי הדלקת – PG2 (ראה טבלה בסוף).
מנגד עודפים בחומצת אומגה 6 תביא לתוצר פירוק נוסף – חומצה ארכידונית (Arachidonic acid), אשר מעודדת יצור פרוסטגלנדינים שליליים כדוגמת PG2. לשם כך נחוץ היחס הנכון עם האומגה 3 (ראה טבלה בסוף).
אומגה 6 מקורות עיקריים במזון:
כל השמנים הצמחיים כגון: שמן תירס, חמניות, סויה, קנולה, זרעי ענבים, נבט חיטה, נר הלילה, המפ (קנביס), שמן שומשום וכן בכל הזרעים והגרעינים, קטניות ודגן מלא. וכאמור נמצאת גם במזונות מעולם החי.
*תוסף תזונה של G.A.L (המופק משמן נר הלילה או מבוראז') המינון המומלץ 300-600 מ"ג ביום.
תפקידים עיקריים אומגה 3 – חומצה אלפא לינולנית – Alpha Linolenic Acid.
-
לטיפול בהיפרכולסטרולמיה + כבד שומני
-
נוגדת דיכאון – יעילה ותורמת להפחתת הסימפטומים בכל הדרגות
-
היפראקטיביות – בעיקר בילדים
-
בעיות קשב וריכוז – ילדים ומבוגרים
-
תמיכה במערכת החיסון – בלקיחה לאורך זמן
-
מפחיתה לחץ דם גבוה ומדללת מעט את הדם
-
מפחיתה תנגודת לאינסולין
-
פעילות אנטי דלקתית – מפרקים, עיכול, לב וכלי דם
-
איזון מערכת הורמונאלית – כולל לבעיות פוריות בגברים ובנשים
-
נוגדת סרטן – בעיקר למניעה כחלק מאורך חיים בריא והפחתת דלקת
-
טיפול ותמיכה במחלות עור – מחלות עור כרוניות
-
תמיכה קוגניטיבית – מפחיתה סיכון למחלות ניוון תאי כגון אלצהיימר
-
התפתחות תקינה של העובר – קריטי למערכת העצבים והמוח של העובר
-
בריאות העיניים – בעיקר מניעת ניוון ראיה
בגופנו היא הופכת לחומצות שומן הנקראות EPA / DHA.
-
חומצה איקוסאפנטאנואית — (Eicosapentaenoic acid) EPA
-
חומצה דוקוסאהקסאנואית — (Docosahexaenoic acid) DHA
ולמעשה מרבית הפעילות הבריאותית מיוחסת ל 2 חומרי מוצא אלו.
חומצת ה A.L.A נמצאת הן במזון מן הצומח והן במזון מן החי, ההבדל הוא שממזון מהצומח גופנו צריך להפיק את ה EPA+DHA (הוא עושה זאת בכבד), ולכן גם טבעונים יכולים להפיק את חומצות השומן החשובות הללו. לעומת זאת מזון מן החי מגיע כבר מוכן עבורנו עם 2 חומצות השומן ובכך הספיגה היא אופטימאלית ובטוחה יותר. חישבו על אנשים שסובלים מתפקוד לקוי של הכבד או כבד שומני, אלכוהוליסטים, חולי צהבת, חולי שחמת וכו', לא בטוח שאצלם הכבד יוכל להפיק את אותן החומצות בכמות מספקת ועל כן החשיבות לקבלן מוכנות וזמינות הינה גבוהה. חשוב לדעת כי בניגוד לאומגה 6, לא נמצאה רעילות או בעיה כלשהי בצריכה עודפת של אומגה 3 גם במינונים גבוהים במיוחד.
אומגה 3 מקורות עיקריים במזון:
מהצומח: אצות, זרעי פשתן, זרעי צ'יאה, אגוזי מלך, סויה, פירות יער.
מהחי: בעיקר דגי מים עמוקים (סלמון*, מקרל, הליבוט, טונה והרינג), ביצים.
*הערה חשובה: 98% מדגי הסלמון שמגיעים לארץ ישראל הינם מגידול בריכות (Farmed salmon) בחופי האוקיינוס ולא דגי בר. מבדיקות שנערכו בשנים האחרונות מסתמן שהם מכילים כמויות גבוהות מאוד של רעלים ומתכות, ניזונים בתערובות מזון גרועות ביותר ולא מאצות ודגי ים טבעיים, מקבלים אסטקסנטין סינטטי לצביעת בשרם בצבע ורוד, מקבלים זרזי גדילה לשקול יותר במכירתם, מקבלים אנטיביוטיקה למניעת זיהומים בכלובים ולשמירת בשרם עד שמגיעים לצלחת ועוד. על כן המלצת המרכז לרפואה טבעית לצרוך רק סלמון אורגני עם חותמת של גוף מוכר או סלמון בר עם חותמת (Wild salmon).
היחס הנכון:
שיעור הצריכה הממוצע של אומגה 3:6 (בעולם המערבי) עומד על יחס של 1:20 לטובת האומגה 6. ובכך למעשה נוצרים עודפים ונזקים מקבוצת ה 6 , ויותר נכון לומר חוסרים מקבוצת ה 3. קל מאוד לסבול מחוסר איזון בתזונת המערב כיוון שהאומגה 6 מצויה בשפע בכל השמנים הצמחים, באגוזים, שקדים גרעינים וזרעים וכן בכל המאכלים מעולם החי. חשוב לדעת שאותו אנזים בגופנו אחראי לפירוק אומגה 3 ואומגה 6, ובכך ח. השומן למעשה מתחרות בינן בגופנו. בשנים האחרונות מחקרים רבים הראו שיחס טוב הוא 1:4 (לטובת האומגה 6) ולאחרונה אף מדברים על יחס של 1:1. יחס זה הוא בר השגה (כמו בטייוואן, יפאן, אסקימוסים) פשוט אין לצרוך שמנים צמחיים כלל מלבד שמן זית (המכיל ברובו אומגה 9 ולא מתחרה עם האומגה 3). ומנגד להרבות באגוזי מלך, במוצרי סויה, זרעי פשתן, צ'יה, אצות ודגי מים עמוקים.
*חשוב לציין שמחקרים הראו שגופנו יכול להמיר את חומצת השומן ALA לחומצות השומן EPA עד 20% ו DHA עד 5% בלבד.
לכן יש יתרון כאן דווקא לתוספי שמן הדגים, שכאמור הם נקלטים בצורה יעילה וזולה וגם מי שאינו חסיד דגים יכול לאזן את היחס בגופו בקלות.
מינונים באוכלוסיות השונות
מינון מומלץ לתחזוקה ע"פ RDA:
הערה: תוספי התזונה המכילים אומגה 3 מגיעים בשלל מינונים ועוצמות שונות (300 מ"ג, 600 מ"ג, 900 מ"ג וכו') החשוב זה לבדוק מהו הריכוז של 2 החומרים הפעילים EPA+DHA סה"כ יחד ולא כמה שמן מכילה הכמוסה ולא את גודל הכמוסה.
ילדים:
עד גיל שנה: 0.5 גרם
1-3: 0.7 גרם
4-8: 0.9 גרם
9-13: 1.2 גרם
נשים:
14 ומעלה: 1.1 גרם
הריון והנקה: 1.4 גרם
גברים:
14 ומעלה 1.6 גרם
*יש לזכור שאומגה 3 מדללת מעט את הדם. מחקרים הראו שעד 3 גרם ליום אתם נמצאים בטווח הבטוח (נוטלי מדללי דם יש להיוועץ במטפל מוסמך).
אגב ישנם עוד 3 חומצות שומן בלתי רוויות שנמצאות בקדמת המחקר והן:
אומגה 5 – חומצת השומן נקראת חומצה פוניסית (Punicic acid), ונחשבת לנוגד חמצון עוצמתי במיוחד. מחקרים בוחנים את השפעותיה על בריאות המוח (במיוחד בהקשר של מחלות ניווניות), איזון רמות הסוכר והשומנים בדם, ואף תכונות אנטי-סרטניות מסוימות.
אומגה 5 נמצאת בריכוז גבוה במיוחד בשמן המופק מזרעי פרי הרימון והיא מהווה כ-65% מחומצות השומן שבו.
אומגה 7 – חומצת השומן נקראת חומצה פלמיטולאית (Palmitoleic acid), נחשבת למשקמת עור מהמעלה הראשונה. המחקרים מתמקדים כיום בהשפעותיה על בריאות העור והריריות, עוד נמצא שהיא מסייעת בהפחתת דלקות, ועשויה לתרום לשיפור הרגישות לאינסולין ולבריאות הלב.
אומגה 7 נמצאת בריכוז גבוה מאוד בשמן המופק מפירות האובלפיחה (פרי כתום וקטן הנפוץ במזרח אירופה) וכן באגוזי מקדמיה.
אומגה 15 – חומצת השומן נקראת חומצה פנטדקנואית (Pentadecanoic acid) או בקיצור C15:0, חומצת שומן בעלת שרשרת אי-זוגית והיא איננה "אומגה" במובן המסורתי של חומצות שומן בלתי רוויות כמו אומגה 3 או 6, אך היא משווקת כחומצת שומן חיונית חדשה התומכת בבריאות התאית.
המחקר מתמקד כיום בהבנה כיצד C15:0 משתלבת בממברנות התאים. נמצא שהיא מחזקת את הממברנות ומגנה עליהן מפני נזק חמצוני הקשור להזדקנות, ומשפרת את תפקוד המיטוכונדריה.
חומצת השומן נמצאת בריכוז גבוה בחמאה ובדגים.
טבלאות עזר
טבלה מס' 1
טבלה מס' 2

טבלה מס' 3

כתיבה: אמיר לוי, נטורופת והרבליסט קליני – מנהל המרכז לרפואה טבעית – www.medicalherbs.co.il
References – מקורות
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014.
- Jones PJH, Papamandjaris AA. Lipids: cellular metabolism. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:132-48.
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.
- Lichtenstein AH, Jones PJH. Lipids: absorption and transport. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:118-31.
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.
- SanGiovanni JP, Chew EY. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res 2005;24:87-138. [PubMed abstract]
- Gabbs M, Leng S, Devassy JG, Monirujjaman M, Aukema HM. Advances in our understanding of oxylipins derived from dietary PUFAs. Adv Nutr 2015;6:513-40. [PubMed abstract]
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med 2008;233:674-88. [PubMed abstract]
- James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc 2010;69:316-23. [PubMed abstract]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. (Prepared by the Tufts New England Medical Center Evidence-based Practice Center, Boston, MA.) AHRQ Publication No. 04-E009-1. Agency for Healthcare Research and Quality, 2004.
- Stanley JC, Elsom RL, Calder PC, Griffin BA, Harris WS, Jebb SA, et al. UK Food Standards Agency workshop report: the effects of the dietary n-6:n-3 fatty acid ratio on cardiovascular health. Br J Nutr 2007;98:1305-10. [PubMed abstract]
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst 2014;106:dju019. [PubMed abstract]
- Fritsche KL. Too much linoleic acid promotes inflammation-doesn’t it? Prostaglandins Leukot Essent Fatty Acids 2008;79:173-5. [PubMed abstract]
- Brasky TM, Till C, White E, Neuhouser ML, Song X, Goodman P, et al. Serum phospholipid fatty acids and prostate cancer risk: results from the prostate cancer prevention trial. Am J Epidemiol 2011;173:1429-39.
- Brasky TM, Darke AK, Song X, Tangen CM, Goodman PJ, Thompson IM, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst 2013;105:1132-41. [PubMed abstract]
- Harris WS, Sands SA, Windsor SL, Ali HA, Stevens TL, Magalski A, et al. Omega-3 fatty acids in cardiac biopsies from heart transplantation patients: correlation with erythrocytes and response to supplementation. Circulation 2004;110:1645-9. [PubMed abstract]
- Harris WS. Are n-3 fatty acids still cardioprotective? Curr Opin Clin Nutr Metab Care 2013;16:141-9. [PubMed abstract]
- Sun Q, Ma J, Campos H, Hankinson SE, Hu FB. Comparison between plasma and erythrocyte fatty acid content as biomarkers of fatty acid intake in US women. Am J Clin Nutr 2007;86:74-81. [PubMed abstract]
- Agency for Healthcare Research and Quality. Omega-3 fatty acids and cardiovascular disease – update. 2015.
- Harris WS, Von Schacky C. The Omega-3 Index: a new risk factor for death from coronary heart disease? Prev Med 2004;39:212-20.
- Harris WS. The omega-3 index as a risk factor for coronary heart disease. Am J Clin Nutr 2008;87:1997S-2002S. [PubMed abstract]
- Metcalf RG, Cleland LG, Gibson RA, Roberts-Thomson KC, Edwards JR, Sanders P, et al. Relation between blood and atrial fatty acids in patients undergoing cardiac bypass surgery. Am J Clin Nutr 2010;91:528-34.
- von Schacky C. Use of red blood cell fatty-acid profiles as biomarkers in cardiac disease. Biomark Med 2009;3:25-32. [PubMed abstract]
- Miller MR, Nichols PD, Carter CG. n-3 Oil sources for use in aquaculture–alternatives to the unsustainable harvest of wild fish. Nutr Res Rev 2008;21:85-96. [PubMed abstract]
- Cladis DP, Kleiner AC, Freiser HH, Santerre CR. Fatty acid profiles of commercially available finfish fillets in the United States. Lipids 2014;49:1005-18. [PubMed abstract]
- Sprague M, Dick JR, Tocher DR. Impact of sustainable feeds on omega-3 long-chain fatty acid levels in farmed Atlantic salmon, 2006-2015. Sci Rep 2016;6:21892. [PubMed abstract]
- Van Elswyk ME, McNeill SH. Impact of grass/forage feeding versus grain finishing on beef nutrients and sensory quality: the U.S. experience. Meat Sci 2014;96:535-40. [PubMed abstract]
- U.S. Food and Drug Administration. Questions & answers for consumers concerning infant formula. 2015.
- U.S. Department of Agriculture, Agricultural Research Service. FoodData Central, 2019.
- National Institutes of Health. Dietary Supplement Label Database. 2015.
- U.S. Food and Drug Administration. Fish: what pregnant women and parents should know. 2014.
- ConsumerLab.com. Product review: fish oil and omega-3 fatty acid supplements review (including krill, algae, calamari, green-lipped mussel oil). 2016.
- Dyerberg J, Madsen P, Moller JM, Aardestrup I, Schmidt EB. Bioavailability of marine n-3 fatty acid formulations. Prostaglandins Leukot Essent Fatty Acids 2010;83:137-41. [PubMed abstract]
- Cunningham E. Are krill oil supplements a better source of n-3 fatty acids than fish oil supplements? J Acad Nutr Diet 2012;112:344.
- Davidson MH, Kling D, Maki KC. Novel developments in omega-3 fatty acid-based strategies. Curr Opin Lipidol 2011;22:437-44.
- Schuchardt JP, Schneider I, Meyer H, Neubronner J, von Schacky C, Hahn A. Incorporation of EPA and DHA into plasma phospholipids in response to different omega-3 fatty acid formulations–a comparative bioavailability study of fish oil vs. krill oil. Lipids Health Dis 2011;10:145.
- Ulven SM, Holven KB. Comparison of bioavailability of krill oil versus fish oil and health effect. Vasc Health Risk Manag 2015;11:511-24.
- Arterburn LM, Oken HA, Bailey Hall E, Hamersley J, Kuratko CN, Hoffman JP. Algal-oil capsules and cooked salmon: nutritionally equivalent sources of docosahexaenoic acid. J Am Diet Assoc 2008;108:1204-9.
- U.S. Department of Agriculture, Agricultural Research Service. What we eat in America, 2011-2012. 2015.
- Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002-2012. Natl Health Stat Report 2015:1-16. [PubMed abstract]
- Black LI, Clarke TC, Barnes PM, Stussman BJ, Nahin RL. Use of complementary health approaches among children aged 4-17 years in the United States: National Health Interview Survey, 2007-2012. Natl Health Stat Report 2015:1-19. [PubMed abstract]
- Papanikolaou Y, Brooks J, Reider C, Fulgoni VL, 3rd. U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake: results of an analysis using observational data from NHANES 2003-2008. Nutr J 2014;13:31. [PubMed abstract]
- Djousse L, Akinkuolie AO, Wu JH, Ding EL, Gaziano JM. Fish consumption, omega-3 fatty acids and risk of heart failure: a meta-analysis. Clin Nutr 2012;31:846-53. [PubMed abstract]
- Del Gobbo LC, Imamura F, Aslibekyan S, Marklund M, Virtanen JK, Wennberg M, et al. Omega-3 polyunsaturated fatty acid biomarkers and coronary heart disease: pooling project of 19 cohort studies. JAMA Intern Med 2016;176:1155-66. [PubMed abstract]
- Wang C, Harris WS, Chung M, Lichtenstein AH, Balk EM, Kupelnick B, et al. n-3 Fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: a systematic review. Am J Clin Nutr 2006;84:5-17.
- Kris-Etherton PM, Harris WS, Appel LJ, American Heart Association. Nutrition C. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002;106:2747-57. [PubMed abstract]
- Burr ML, Fehily AM, Gilbert JF, Rogers S, Holliday RM, Sweetnam PM, et al. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: Diet and Reinfarction Trial (DART). Lancet 1989;2:757-61.
- Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999;354:447-55. [PubMed abstract]
- Marchioli R, Barzi F, Bomba E, Chieffo C, Di Gregorio D, Di Mascio R, et al. Early protection against sudden death by n-3 polyunsaturated fatty acids after myocardial infarction: time-course analysis of the results of the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico (GISSI)-Prevenzione. Circulation 2002;105:1897-903. [PubMed abstract]
- Morris MC, Sacks F, Rosner B. Does fish oil lower blood pressure? A meta-analysis of controlled trials. Circulation 1993;88:523-33. [
- Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Saito Y, Ishikawa Y, et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet 2007;369:1090-8. [PubMed abstract]
- Tanaka K, Ishikawa Y, Yokoyama M, Origasa H, Matsuzaki M, Saito Y, et al. Reduction in the recurrence of stroke by eicosapentaenoic acid for hypercholesterolemic patients: subanalysis of the JELIS trial. Stroke 2008;39:2052-8. [PubMed abstract]
- Risk and Prevention Study Collaborative Group, Roncaglioni MC, Tombesi M, Avanzini F, Barlera S, Caimi V, Longoni P, Marzona I, Milani V, Silletta MG, Tognoni G, Marchioli R. n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013 May 9;368(19):1800-8.
- ORIGIN Trial Investigators, Bosch J, Gerstein HC, Dagenais GR, Diaz R, Dyal L, et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med 2012;367:309-18. [PubMed abstract]
- Kromhout D, Giltay EJ, Geleijnse JM, Alpha Omega Trial Group. n-3 fatty acids and cardiovascular events after myocardial infarction. N Engl J Med 2010;363:2015-26. [PubMed abstract]
- Bowman L, Mafham M, Wallendszus K, Stevens W, Buck G, et al.; ASCEND Study Collaborative Group. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus.N Engl J Med 2018;379:1540-50.
- Manson JE, Cook NR, Lee I-M, Christen W, Bassuk SS, Mora S, et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N Engl J Med. 2018 Nov 10. doi: 10.1056/NEJMoa1811403. [Epub ahead of print] [PubMed abstract]
- Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11-22. [PubMed abstract]
- Kris-Etherton PM, Richter CK, Bowen KJ, Skulas-Ray AC, Jackson KH, et al. Recent clinical trials shed new light on the cardiovascular benefits of omega-3 fatty acids. Methodist Debakey Cardiovasc J 2019;15:171-8.
- Rimm EB, Appel LJ, Chiuve SE, Djoussé L, Engler MB, et al.; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Seafood long-chain n-3 polyunsaturated fatty acids and cardiovascular disease: a science advisory from the American Heart Association. Circulation 2018;138:e35-
- Hu Y, Hu FB, Manson JE. Marine omega-3 supplementation and cardiovascular disease: an updated meta-analysis of 13 randomized controlled trials involving 127 477 participants. J Am Heart Assoc 2019;8:e013543.